 English
English Turkish
Turkish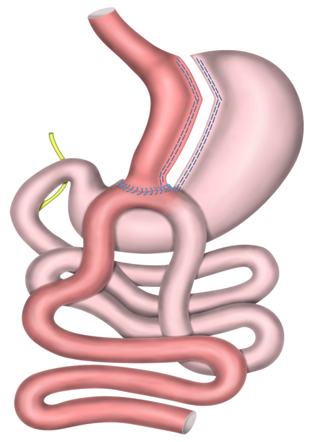
Mini-Gastric Bypass (MGB)
Mini Gastric Bypass (MGB) obesity surgery is the easiest, shortest and most economic gastric bypass operation with the shortest hospitalization period. Mini Gastric Bypass operation provides a weight loss obtained with standard gastric bypass operations. This operation has a strong control over Type 2 Diabetes, hypertension (high blood pressure), hyperlipidemia (elevation in cholesterols) which are main accompanying findings of Metabolic Syndrome.
How is Mini Gastric Bypass Applied?
Mini gastric Bypass is a malabsorptive obesity surgery which reduces gastric volume and decreases food absorption from small intestines. Its fully laparoscopic. 4 to 5 skin incisions which are smaller than 1 cm are applied. The camera and operation devices are placed from these incisions. Camera and operation tools used are specific tools which are designed smaller and thinner for convenience of passing through these port sites. A small gastric tube is created at stomach orifice and it is completely separated from the remaining stomach. The actual stomach which will be used after the operation is the new stomach part which has been shaped like a tube. No organ is removed. The larger part of the stomach stays dysfunctional in the abdomen and continues to produce secretions.
The small stomach which was newly created is connected with small intestine and a new route for food is established. This part is the second stage of the operation. A new path is reconstructed onto the new stomach and approximately the proximal 2 m of the small intestine is bypassed and a connection onto the middle part of small intestine is applied.
How is stomach and small intestine connected to each other?
This anastomosis is accomplished by special staplers. These staplers are specific tools produced for laparoscopic surgery. It is placed into the stomach and small intestine which stay adjacent and closed. It adheres stomach and small intestine and creates a space to provide passage. This connection is called anastomosis.
Anastomosis means connection of two empty organs together. When an organ or a part of an organ is removed in the digestive system, remaining two ends are always connected with an anastomosis.
We use stapler in some stages of the surgery. However, we do not use it to connect stomach and small intestine on anastomosis part. We perform the connection between the stomach and intestine by hand sown sutures.
What is superiority of anastomosis performed by hand?
You feel each millimeter of tissue sutured when you perform hand sown anastomosis. You do not leave any weak or loose area in this case. This minimizes leakage possibility in anastomosis. Therefore, we start liquids at the same day of surgery.
How Do I Loose Weight By mini-Gastric Bypass?
Weight loss by Mini-gastric bypass occurs via three ways:
Gastric Volume Restriction:
- Your gastric volume is reduced with mini-gastric bypass. Your meal portions reduce with this new reduced stomach. Frequincy of the meal that you eat increase. It has a similar effect with sleeve gastrectomy. However, a larger gastric tube is created in sleeve gastrectomy operation. So, a stronger volume restriction is done in Mini Gastric Bypass operation.
Malabsorption:
- About 200 cm of proximal part of small intestines is separated from food passage in mini-gastric bypass operation. This bypassed jejunum carry bile and pancreatic juices which provide digestion and absorption. Foods are transferred into the middle section of small intestine after they pass from small stomach. Mixing with bile is provided at this stage. Complete absorption starts after first 200 cm.
- Blockage of food passage from first 200 cm of small intestine prevents food absorption from these part. Excessive calories are discharged without absorption. This malabsorptive effect provides high weight loss quantity and preserving this weight loss for a long period.
Hormonal Regulation:
- Most of the stomach is bypassed in Mini-gastric Bypass operation. Foods taken do not pass to this section. So, this part is not stimulated by foods and looses its efficiency slowly. It has been reported that hunger hormone secreted from such part has partially decreased. Decrease of ghrelin, the hunger hormone provides to have fullness earlier. Furthermore, period of fullness prolongs.
Mini Gastric Bypass and Risks
Bile reflux
The most important problem with Mini Gastric Bypass is the bile reflux to the stomach pouch. This ratio is reported very small in articles and different series reported. However, alkaline reflux causes severe symptoms and decreases quqlity of life.
To reduce or eliminate this reflux, the intestine part carrying bile secretion into the anastomosis is connected proximally to the stomach. This technique claims to create a disposition for bile flow to continue in the small intestine without passing inside the stomach. But we observe the bile reflux not at the early periods but after a year.
How is Bile Reflux Treated?
We apply stomach protective treatments for patients operated who have bile reflux complaints. We routinely prescribe stomach protecting syrups and sometimes drugs for first 6 months for our patients even without any complaint. Complaints may be much in some cases. It may become continuous during night and day. In these cases, some surgical changes may be necessary.
- Brown Anastomosis: A distal connection might be done between the biliopancreatic limb and common channel more than 150 cm diatal to gastrojejunal anastomosis. This aims to provide bile flow directly into the distal small intestine part without entering the stomach. The procedure is very short. The operation is performed laparoscopically. But our experience shows that it is mostly inefficient to control bile reflux.
- R-Y Gastric Bypass: Complaints may not disappear by Brown Anastomosis in some patients. In this case, Mini Gastric Bypass operation may be required to convert to R-Y Gastric Bypass. So, bile flow is separated from the stomach definitely with a separate tract.
- Duodenal Switch: It is an ideal reconstruction method. It is more ideal to perform duodenal switch first for many patients. However, some of the patients hesitate to have switch operation because of misinformation. Duodenal Switch operations are the most ideal revisional surgical methods after unsuccessful mini gastric bypass operation. The pylorus muscle which was bypassed with mini gastric bypass is preserved and actively used. Furthermore, no dysfunctional stomach part which has gastric cancer risk is left behind. The new stomach may be accessed easily after duodenal switch operation.
Gastric ulcers: It may be observed in patients who have bile reflux longer. It appears on anastomosis line (where stomach and intestine is connected). It is followed by proton pump inhibitors, sucralfate and frequent endoscopic control. If no recovery appears within 2 to 3 months, surgical reconstruction may be necessary. In this case, R-Y Gastric Bypass or Duodonal Switch will be a valid alternative.
Dumping Syndrome: Like all bypass operations, much liquid passes into the intestines when much carbohydrate is taken. So much liquid in the stomach causes bloating and tension in the stomach. Furthermore, blood pressure also decreases because vascular fluid reduces. Severe nausea and vomiting and syncope accompanies to this phenomenon.
The main cause for Dumping Syndrome is deactivation of the muscle system called Pylorus which controls gastric exit after mini gastric bypass operation. As the pylorus muscle is deactivated, bile flows downwards in contact with the stomach without any barrier. Therefore, mini gastric bypass has the highest risk for bile reflux.
Starchy foods should be avoided to prevent Dumping Syndrome. Foods including white flour and starch should not be eaten. White bread, pita and thin bread, pasta and bakery products are included in this group.
Standard Risks of Gastric Bypass Operations
- Severe Biliary Reflux
- Vitamin and mineral deficiencies due to malabsorption.
- Sometimes diarrhea due to shorter intestinal distance,
- Osteoporosis,
- Insufficient or excessive weight loss,
- Nausea- Vomiting,
- Anastomosis leakage,
- Abscess or wound infection,
- Deep Vein Thrombosis,
- Pulmonary embolism,
- Fistula,
- Gall bladder or bile duct stones
- Stenosis on anastomosis,
- Partial or complete intestinal obstructions due to intra-abdominal adhesions,
Does Mini Gastric Bypass Cause Gastric Cancer?
Mini Gastric Bypass connects the newly formed gastric pouch to jejunum in a loop fashion anastomosis. This means the bilio-pancreatic juice is not diverted distal from the pouch. Although some technical maneuvers are proposed that claim to reduce and/or prevent bile reflux; it is very frequent to observe significant bile stains or severe biliary content in small gastric pouch after MGB. We must admit that, chronic biliary reflux to stomach and esophagus is definitely a risk factor for canser formation in long term. This is the main concern for gastric pouch.
MGB or RYGB both do not increase the cancer formation risk in the remnant stomach.
What is Disadvantage of Mini Gastric Bypass Operation?
The most significant disadvantage of mini gastric bypass is that, the risk of biliary reflux to gastric pouch. Also passive stomach can not be monitored by endoscopy in terms of cancers that may develop during further years. This problem is also valid for Roux-en-Y Gastric Bypass operation where the stomach is left. However, there is not such risk because no passive stomach is left in BPD/DS, Duodenojejunal Bypass or Duodenoileal Interposition.
